

The Committee on Tactical Combat Casualty Care (CoTCCC) added Suzetrigine as an option for initial analgesia in their updated TCCC guidelines in May 2026. However, despite suzetrigine already being on formulary in DOD treatment facilities, there is little established use in medical sets or in garrison clinics yet. Therefore most military medics may be asked to incorporate suzetrigine without any experience or significant training (or experience from their supervising PAs or physicians). This article will use a Q&A format to provide medics, their NCOs, and providers with a way to become familiar with suzetrigine for patient care in training and forward operations.

Authors: Collin D, PA-S, SOCM
Co-authors: Brandon C, DSc, PA-C
“What is suzetrigine, anyways?”
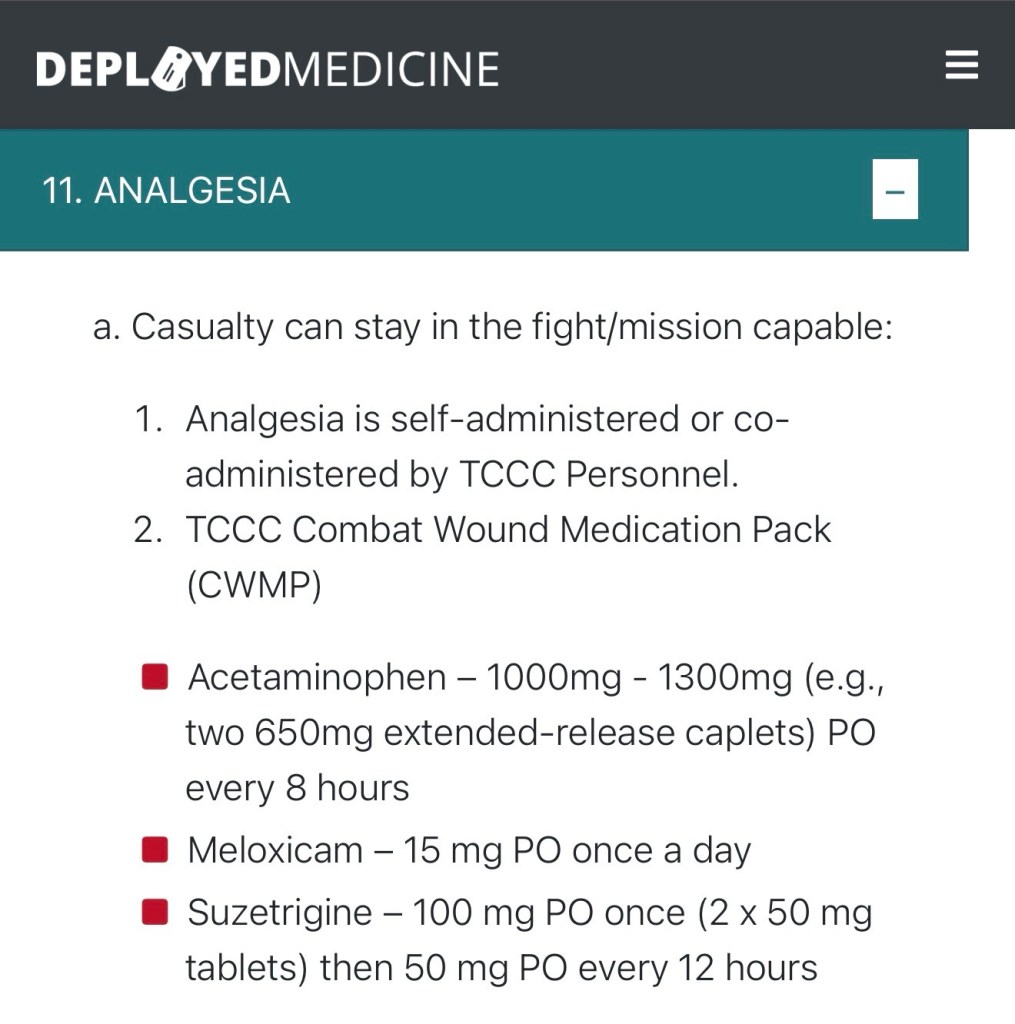
The short answer is that suzetrigine is a non-opioid tablet currently recommended by CoTCCC to treat casualties with mild to moderate pain. The initial oral dosing is 100mg (2x 50mg tablets), followed by 1x 50mg tablet up to every 12 hours as needed.
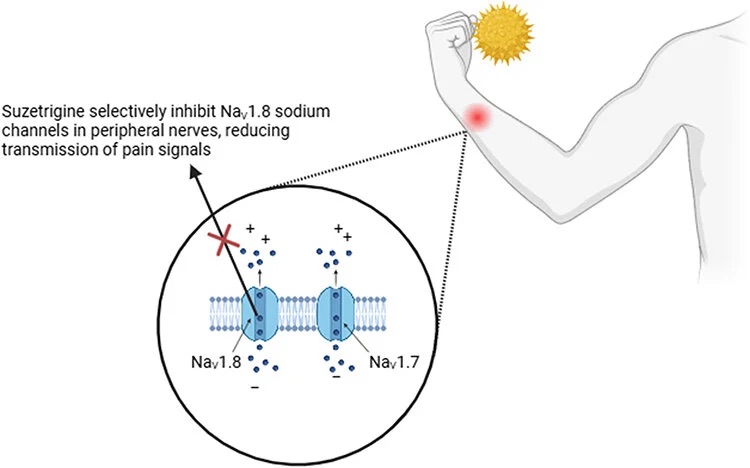
The long(er) answer is that suzetrigine functions as a uniquely selective “circuit breaker” for peripheral nerves by blocking the action potential sodium channel “NaV1.8” (“Na” is the elemental symbol for sodium), which is found in the dorsal root ganglion (“the brain center” of the nerve). The selectivity of suzetrigine for the NaV1.8 channel without noted effects on other channels helps to avoid unwanted side effects, particularly of the central nervous system (CNS) as well as with other selective sodium channels like NaV1.5 (which affects cardiac rhythm) and NaV1.4 ( which can affect motor function). In one study, researchers found that suzetrigine had more than 31,000-fold selectivity ratio for NaV1.8, and less than 0.1% inhibition of other NaV channels.
While a medic shouldn’t necessarily memorize all the specifics of the mechanism of action, it should be understood that suzetrigine works in the peripheral nerves rather than centrally (like the brain), but is not exclusive to a single local area, like a lidocaine injection. Clinically, this “peripheral-rather-than-central” mechanism helps to understand that this medication can be given and not hinder combat effectiveness in a casualty, unlike medications that target the CNS for pain control, and thus have higher side effect profiles, like ketamine, morphine, or fentanyl.
“When do we use suzetrigine? I mean, we already have Ketamine?”

CoTCCC recommendations still include ketamine and Esketamine, however it is for moderate to severe pain in casualties that are already combat ineffective. Suzetrigine instead is recommended as an option primarily for those who can remain in the fight but need more help than acetaminophen (Tylenol) and meloxicam (Mobic) can provide. Given its prolonged onset and extended duration (half-life measured at approximately 24 hours), suzetrigine also creates an attractive option to conserve resources with ketamine or opioids in potential prolonged casualty care (PCC) situations.
Without suzetrigine, casualties still combat effective are limited to acetaminophen and meloxicam. For those not effective, or disarmed due to ketamine, their only option would be continued IV push of Ketamine, setting up complicated TIVA drips, or training on additional medication.
As an oral medication, we are assuming that the treated casualty does not have injuries or issues that could make an oral route risky, such as facial trauma, inability to protect airway and more. In those cases, following CoTCCC recommendations and TCCC guidelines should first address these potential life threats, and use primarily IV/IO medications for analgesia.
A combat medic could also give this to a patient that is experiencing moderate pain that is not from war wounds (DNBI), but is impacting their ability to continue the mission. This must be discussed with Unit BN PA/MD for training and approval.
“What does giving Suzetrigine look like? I don’t know how long it will take to kick in, and what that looks like?”

A patient given suzetrigine orally can start expecting some pain relief within 30-60 minutes, with a peak at 2-3 hours if on an empty stomach. Patients who have recently eaten may see a peak analgesia level around 5 hours.
The initial dose is 100mg (two 50mg pills). Follow-on doses are 50mg (one pill) every 12 hours thereafter. Use beyond 14 days has not been studied extensively, but a combat medic should definitely be in contact with a higher-level provider well before that to consider continued management with suzetrigine, transition to other medications, or underlying pathology contributing to their pain.
It is also recommended suzetrigine NOT be crushed since it may impact absorption, which means it is not a viable consideration for NG/OG tube administration in PCC.
“What side effects do they have at normal doses, or if accidentally given too much?”

Side effects are generally mild in both severity and complexity, including dizziness, nausea, itching, and potential muscle spasms. However, in prior trials of postsurgical pain treatment, rates of adverse events of nausea, vomiting, dizziness, and headache were all significantly lower in those taking suzetrigine vs. norco (hydrocodone-acetaminophen). Overall, given that the intent is to treat a casualty with suzetrigine and remain combat effective, this decreased side effect risk is outweighed by the potential benefit of analgesia..
Nausea is by far the most common side effect (in one trial, it constituted about half of all reported side effects) and since this is a relatively mild concern, a medic should remember to readily utilize ondansetron (Zofran), either sublingual, or IV to help mitigate this concern. Stronger analgesic options (like morphine or ketamine) are more likely to induce nausea, and so ondansetron should always be considered as an adjunct treatment during TCCC training, as well.
Advanced: Suzetrigine is an inducer of CYP3A, an enzyme primarily made in the liver that helps metabolize (break down) medications. This means that if casualties are taking other medications that are metabolized by CYP3A, there can be some interference with the metabolism of suzetrigine. Most of the medications recommended by CoTCCC for use in the prehospital environment do not create concerns regarding the CYP3A enzyme, with the exception of midazolam. Midazolam is metabolized by CYP3A, and its effectiveness may be potentially lessened with simultaneous use of suzetrigine. Conversely, if medications cannot be metabolized because of a chemical back-up with CYP3A, their concentrations may be increased in the blood, leading to toxicity concerns. This may mean dosing may need to be adjusted accordingly.
“Can this be used with other medication? (Ketamine, Tylenol, etc)”
Suzetrigine is intented to be used with other medications; it can be given with acetaminophen and/or an NSAID such as meloxicam (Mobic), assuming the patient has no contraindications to either of those. This could mean suzetrigine is given with, before, or after these medications.
Additionally, acetaminophen can be redosed sooner than suzetrigine, and some patients may respond well enough to the acetaminophen doses after in order to wean off and conserve use of suzetrigine over prolonged periods.
Due to longer durations of analgesia, suzetrigine may help create a synergistic effect with other medications to use less ketamine and/or opioid in a patient being given those for pain, but able to safely tolerate oral medication. It may also help wean them off those medications if the suzetrigine alone can manage their pain.
The TCCC guidelines do mention either 2x 500mg or 2x 650mg extended release acetaminophen tablets every 8 hours (posted below), which still keeps them under 4,000mg a day for safety. Keep in mind typical dosing for prolonged periods of acetaminophen use is 500mg x2 every 8 hours, not to exceed 3G a day for chronic use, when used in sick call.
“How do I implement Suzetrigine into TCCC and PCC training?”

First, TCCC training should NEVER include verbalizing medication. Medics do not get enough experience in hospitals and ambulances to skip precious physical repetitions in training. Medics should always be expected to use 10mL saline vials (NSN: 6505-01-287-0626) with a fake label to represent ketamine, TXA, and other medications during lanes. In the case of oral meds such as suzetrigine, ondansetron, acetaminophen and more, a pill bottle or other labeled container (medication bag or small box with dividers from Amazon) with a small edible candy such as “Tic Tac” to administer to the roleplayer (or manikin) can suffice.
- Giving meds instead of verbalizing gets medics used to the proper dose and WHERE they carry meds in their aid bag, shoulder sleeve or combat belt. Medics will therefore be able to distinguish between first-time dosing of suzetrigine (two pills) vs. subsequent doses (one pill) and the proper timing intervals. They also need to know how to pair this with other medications they carry on them.
- Proctors should watch intently whenever medics are dispensing medication for 5+ rights violations. The initial dose for suzetrigine is two pills. Giving one pill, or three pills, especially without a specific reason is considered improper dosing and should be handled accordingly. More mistakes tend to happen with syringes, as even verbalization of the right dose might mean drawing up another dose.
- This is also a chance to see what your medics will pack on patrols/operations, besides suzetrigine. Do they plan to carry acetaminophen, meloxicam, loperamide, and/or sublingual ondansetron? Can they name the doses, indications and contraindications? Do they have name, dose and expiration date written down? All things a senior medic/PA should expect a medic to recite when asked about a medication they carry. Otherwise, it should be temporarily removed from only that individual’s meds (not the unit) until they can recite the information required to make senior medics/providers comfortable for them to administer. Perhaps they can give a class on the medication to the other medics the next day.
- Suzetrigine alone shouldn’t solve the problem every single time. Medics should eventually be challenged with scenarios where the patient may need ketamine after they are given suzetrigine if it becomes more painful, or to give suzetrigine following an initial dose of acetaminophen and meloxicam if those medications are not working.
- Since suzetrigine and other pain management medications (ketamine, fentanyl) have a significant chance to cause nausea, instructors should give simulated casualties nausea beyond just head injuries. Medics should be prepared for this and consider giving ondansetron ODT (Zofran) during training. This assumes they remembered to pack nausea medication like ondansetron for a trauma lane. Alternatively, they could have the patient sniff an alcohol wipe (not verbalize, but physically demonstrate) for a few minutes to keep nausea at bay until ondansetron is drawn up, or placed a properly labeled simulated “medication” (like a Tic-Tac or other piece of candy) under the tongue.
- The time from the first dose of suzetrigine until the second is 12 hours, so it would take a lengthy PCC lane for medics to experience proper redosing intervals. For that reason, before ending a shorter trauma lane, you could ask them when their next dose of suzetrigine is and how much (Only one pill, or 50mg). This also helps them understand that if a patient is complaining about pain in the next few hours, that another dose is not on the table according to guidelines. They must choose another medication, as well as consider why the patient is experiencing new breakthrough pain (compartment syndrome, transportation movement on injuries, etc) and therefore whether or not additional interventions are needed.
- It’s also worth discussing with medics when to consider suzetrigine for patients who have moderate to severe pain that is NOT from war wounds (DNBI), in order to enable them to continue their mission. This may change depending on how much suzetrigine is available, a medics own competency, and threshold for treating. This should not be given by a medic for a DNBI without telemedicine/consult to their BN PA or other provider, unless specifically trained or enabled through proper channels, memorandums and more. For more examples of enabling medics to get more comfortable with sick call operations and medication, read our guide to running sick call.
If you have any corrections or additions, please reach out to us by email or instagram!
References:
- Bertoch T, D’Aunno D, McCoun J, et al. Suzetrigine, a Nonopioid Na V 1.8 Inhibitor for Treatment of Moderate-to-severe Acute Pain: Two Phase 3 Randomized Clinical Trials. Anesthesiology. 2025;142(6):1085-1099.
- 2026 TCCC Guidelines, Deployed Medicine: TCCC Guidelines http://deployedmedicine.com/content/40
- Osteen JD, Immani S, Tapley TL, et al. Pharmacology and Mechanism of Action of Suzetrigine, a Potent and Selective NaV1.8 Pain Signal Inhibitor for the Treatment of Moderate to Severe Pain. Pain Ther. 2025;14(2):655-674.
- Sibomana, O., Okereke, M., & Hakayuwa, C. M. (2025). Suzetrigine Approval Breaks a 25-Year Silence: A New Era in Non-Opioid Acute Pain Management. Journal of Pain Research, 18(0), 2805–2808.

Leave a comment