

A 35-year-old active duty male presents with sudden onset of pain and decreased vision of the right eye, after he was in an altercation (but you can also see this in blast injuries or other objects hitting in this area.) The patient’s exam includes worsening visual acuity of 20/200 (OD), an afferent pupillary defect, worsening proptosis, decreased extraocular movements (note patient is looking down but injured eye stays fixed.)
1.) What is going on with this patient?
2.) Is this stay and play or load and go?
3.) What do you carry to do visual assessments in the field? If you don’t carry anything, how can you test this soldiers acuity?
4.) What other assessments / info would you do?
5.) What is an afferent pupillary defect; How can you tell?
6.) What can we do about it?
STOP. Integrity check.
Don’t continue until you have written down your answers. This integrity check will keep you honest on what you did know or did not, more than just scrolling below to the answers. At a minimum, say out loud what you would do or type it into your phones notes app. Getting negative feedback will help this lesson stick more into memory.
Were your answers close or different to:
1.) What is going on with this patient?
Retrobulbar hematoma; Trauma behind the eyeball has caused blood to push on the eye and optic nerve, causing orbital compartment syndrome.
2.) Is this stay and play or load and go?
Aggressively evacuate, “Life, Limb or EYESIGHT.”
3.) What do you carry to do visual assessments in the field? If you don’t carry anything, how can you test this soldiers acuity?
Some medics may consider small snellen charts for field visual assessments, weighs next to nothing and allows you to get a baseline ( or if they are your soldier know their baseline) and catch trending of worsening vision. 
Pictured is the “Maxwells Quick Medical Reference”, an example of a small handheld reference with multiple uses; snellen chart included.
A medic can also make their own by printing of a snellen chart onto a small 3 in x 5 in or equivalent card and then laminating it to go with your eye shields and other eye injury supplies.
If you do not have either of those during an eye injury, try to find a reference, guide or paper with different sizes of writing. While these methods aren’t accurate for calculating their actual vision, it can be used to try to catch “Are they getting worse or staying the same?”
4.) What other assessments / info would you do?
Other clinical eye exams would be useful, but keep in mind if the Mechanism of Injury is a blast, not a punch/object to the face, then we shouldn’t get tunnel visioned on a nasty looking eye.
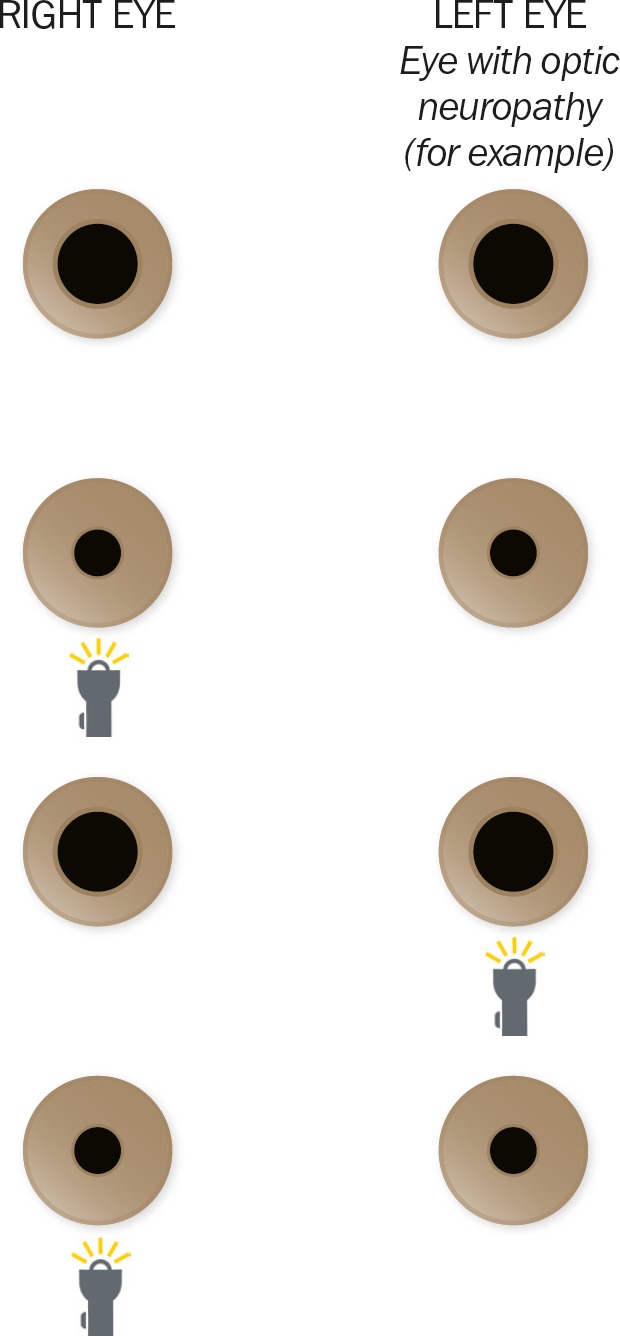
5.) What is an afferent pupillary defect; How can you tell?
Relative afferent pupillary defect (RAPD):
–> Click here for how to do a “Swinging Light Test” to look for RAPD, why to do one, and why it works <—
“What can we do about a retrobulbar hematoma?”
At minimum, a medic needs to recognize this early to be sent up to higher. There is little we can do, even surgical interventions buy time for them to get higher. By letting the next echelon know about this condition they can already have their kits ready to perform this earlier and expect to receive this patient.
Advanced: What procedure is used to relieve this? Do you have the means to perform this out of an aid bag?
 The Lateral Canthotomy is a surgical procedure only to be performed by trained medical professionals, usually advanced combat medics or SOF. In an austere situation this may buy your patient time so they do not lose their eyesight permanently.
The Lateral Canthotomy is a surgical procedure only to be performed by trained medical professionals, usually advanced combat medics or SOF. In an austere situation this may buy your patient time so they do not lose their eyesight permanently.
In the event of extended medical evacuation, the medic may have to call and ask permission from higher authorities to perform the procedure, especially if untrained. If it is indeed a confirmed retrobulbar hematoma, the patient will most likely lose the eyesight if no intervention is performed, versus the procedure may help if done correctly. This scope of practice needs to be addressed by your unit.
Here is a video on demonstration and walkthrough on an actual patient:
For further reading, “Taming the SRU” has a good article on this:
http://www.tamingthesru.com/blog/annals-of-b-pod/ocular-emergency
If you haven’t practiced this procedure in awhile, consider implementing it into pre-deployment training, as well as watching multiple videos of how it’s done to freshen up. Besides the ones we posted there are quite a few ones on living and cadaver patients. Have your medics watch the videos as homework before coming in to practice.
Don’t believe medics can perform lateral canthotomy and there is no benefit? Check out this article by Journal of Special Operations Medicine:
Lateral Canthotomy in Orbital Compartment Syndrome: Special Operations Medics on the Battlefield Can Save the Eye

Leave a comment