

Welcome to “Next Gen Shorts”, where we look to take a recent study
focused on military and prehospital medicine, and condense it into a quick
manageable read to ensure you get what’s most important for your practice.
Today’s paper discusses whether the use of ketamine in prehospital trauma increases patient mortality.

The Background:
Ketamine is well-known as an incredibly versatile medication for analgesia and sedation, further supported by hemodynamic stability compared to opioid-based medications. These include less incidence of respiratory depression and hypotension, both of which are paramount when dealing with polytrauma, pulmonary injuries, and possibly hemorrhagic shock.1 As of November 2020, new changes to Tactical Combat Casualty Care (TCCC) guidelines recommend the use of ketamine to treat moderate-to-severe pain in the prehospital environment, increasing recommended doses in part based on the level of the treating provider.2

Traditional thinking has pushed against the use of ketamine in suspected or known head injuries due to stated concerns for increasing intracranial pressure (ICP). Though attempts are consistently made to turn away from this sentiment, reluctance still exists in some circles. Support for this thinking largely comes from scattered case reports of complex patients with established underlying obstructive pathology rather than acute trauma brain injuries (TBI).3 In stark contrast, modern reviews of ketamine find significant neuroprotective effects occur to support its use as analgesia in TBI patients.4
However, the question in the end that many want to know tries to separate statistical significance from actual clinical significance for head injury patients in the prehospital setting (i.e. increased mortality).
The Paper:
Bebarta VS, Mora AG, Bebarta EK, et al. Prehospital use of ketamine in the combat setting: A sub-analysis of patients with head injuries evaluated in the prospective life saving intervention study. Mil Med. 2020 Jan 7;185(Suppl 1):136-142. PMID: 32074369.

The Question:
Do combat casualties with TBI who receive ketamine have increased mortality to compared to those with other analgesia (OA) or no analgesia (NA)?
What the Researchers Did:
- A retrospective search of the Life Saving Intervention (LSI) study, a prospective, observational study of prehospital interventions on combat casualties in Afghanistan from November 2009 to March 2014
- Used patients with analgesia data (October 2012 to March 2014)
- Identified casualties with suspected TBI using abbreviated injury scale (AIS) codes to identify head, neck and/or face injuries
- Outcomes included: 1) discharge home, 2) continued medical care, 3) deceased, and 4) unknown
Demographic Results:
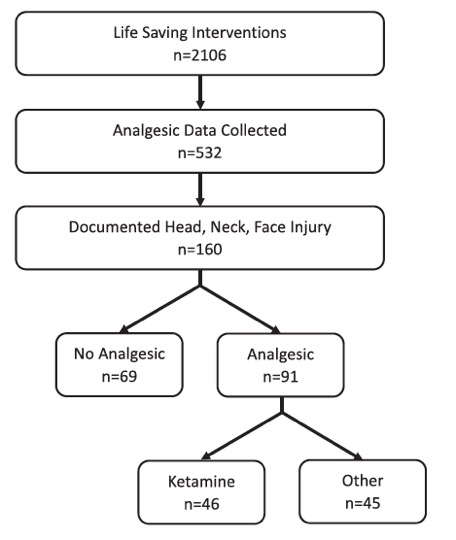
- 2,106 subjects in LSI database
- 532 records with analgesic data
- 160 records with AIS for head, neck, and/or facial injuries
- Most (66%) were injured by explosive, followed by penetrating (21%) and blunt (16%) trauma
- Median injury severity score (ISS) = 12
Research Question Results:
Comparing NA to Ketamine:
- No difference in mortality (OA = 5, Ketamine = 4, p = 0.1819)
- No difference in number of hospital days between groups
- Patients receiving ketamine were more likely to be discharged to continued medical care
Comparing OA to Ketamine:
- No difference in mortality (OA = 2, Ketamine = 4, p = 1.0000)
- No difference in number of hospital days between groups
- Patients receiving ketamine were more likely to be discharged to continued medical care
Conclusion:
Use of ketamine for prehospital analgesia in patients with suspected TBI does not increase mortality rates.
Medic Bottom Line:
Historical case reports warn of increased ICP when administering ketamine, which has become dogma in some circles to advocate against its use in TBI, despite increasing evidence to the contrary. This battlefield-based study further supports that ketamine does not significantly increase mortality compared to other forms of analgesia, or no analgesia. These findings only reinforce and support current TCCC recommendations for the prehospital use of ketamine in trauma.

References
- Gaydos SJ, Kelley AM, Grandizio CM, Athy JR, Walters PL: Comparison of the effects of ketamine and morphine on performance of representative military tasks. J Emerg Med 2015; 48: 313–24.
- Tactical Combat Casualty Care (TCCC) Guidelines for Medical Personnel. 05 November 2002. Accessed 01 February 2021 at: https://learning-media.allogy.com/api/v1/pdf/9e7beef5-e713-472f-9eb3-1f7f0fdf33a3/contents
- Wyte SR, Shapiro HM, Turner P, Harris AB: Ketamine-induced intracranial hypertension. Anesthesiology 1972; 36: 174–6.
- Cohen L, Athaide V, Wickham ME, Doyle-Waters MM, Rose NG, Hohl CM: The effect of ketamine on intracranial and cerebral perfusion pressure and health outcomes: a systematic review. Ann Emerg Med 2015; 65: 43–51e2.

Leave a comment