
Hyponatremia is usually associated with hypoosmolality and most often the result of impaired diluting capacity and inappropriately elevated ADH. There are four factors that are associated with hyponatremia 1) presence of antidiuretic hormone (ADH), 2) insufficient solute intake, 3) excessive free water intake, and 4) impaired urine diluting capacity. ADH is produced in the Supraoptic nucleus Paraventricular nucleus of the hypothalamus and secreted from the posterior pituitary. Any physiologic or pathophysiologic state which causes release of ADH from the posterior pituitary results in the following:
- Decreased urinary water excretion and concentration of the urine
- Increase in total body water content
- Decreased plasma osmolality.
Sodium does not control sodium concentration, water controls sodium concentration. This occurs via aldosterone promotes increased total body sodium content, this causes an increased mean arterial pressure (MAP) and overall volume status. ADH promotes the reabsorption of free water and decreases serum sodium concentration and plasma osmolality.
Salt and water are only connected at steady state. Steady State is when the salt (sodium) and water balance results in one MAP (Figure 1). The normal osmolality of the body is between 275-295 mOsm/kg. The normal sodium level in the body is 135-145 mEq/L.

Figure 1. Steady state
There are Five nephron functions are responsible for the kidney’s ability to achieve maximally dilute urine. Any or all of these functions may contribute to impaired urine diluting capacity and generation/maintenance of hyponatremia:
- 1. Glomerular filtration rate (GFR) needs to be preserved.
- May be decreased by: chronic kidney disease and use of NSAIDs, ACEIs, or ARBs.
- 2. Proximal tubule should not be in a sodium avid state.
- Avid sodium reabsorption occurs in the setting of volume depletion, hypotension, and decreased renal perfusion.
- Thiazide diuretics also cause increased proximal tubule Sodium reabsorption as a secondary effect.
- Activity of the sodium‐potassium‐2 chloride channel (Na‐K‐2Cl) in the thick ascending limb of the loop of Henle (TAL) needs to be preserved.
- The Na‐K‐2Cl channel is blocked by loop diuretics, for example: furosemide, bumetanide, torsemide and ethacrynic acid.
- Activity of the sodium‐chloride cotransporter (NaCC) in the distal tubule needs to be preserved.
- NaCC is blocked by thiazide diuretics, for example: hydrochlorothiazide, metolazone, chlorothiazide, chlorthalidone.
- There should be no water reabsorption at the level of the cortical collecting duct.
- In the setting of hyponatremia and hypo‐osmolar states, when serum osmolality is less than ~280 mOsm/kg, there should be no ADH present in the serum. Furthermore, there should be no activity of ADH at the V2 receptor in the cortical collecting duct.
To evaluate hyponatremia and develop a differential diagnosis, you need to divide the causes into hypovolemic, euvolemic, and hypervolemic. This is possible because you can have hyponatremia with any volume status. There are three causes of hyponatremia that do not present with hypoosmolality.
Pseudohyponatremia is a condition of hyperglobulinemia or hypertriglyceridemia. There is a decreased plasma water as compared to plasma solids. This in turn makes sodium concentration appear low.
Hyperglycemia is a true hyponatremia with a hypertonicity state. This can be seen with the administration of mannitol given to a casualty with a head injury. The molecules increase the osmolality, pulling water out of the cell and dilutes the sodium concentration. For every increase in 100 mg/dL of glucose or mannitol, the sodium falls by 1.6 mEq/L. This increased tonicity causes a release of ADH and also increases thirst. Both will cause water retention.
A third cause of hyponatremia without hypoosmolality is the addition of an isoosmotic non-sodium containing fluid to the extracellular space. This occurs during prostate surgery when large amount of non-conducting solution containing glycine or sorbitol is absorbed by the body.
The ability to achieve adequate free water clearance and avoid the development of hyponatremia involves three factors:
- Preserved urinary diluting capacity
- Adequate daily solute excretion
- Avoidance of excessive free water intake.
Hyponatremia is typically caused by issues: inappropriate ADH and impaired urine diluting capacity. However, there are three diagnoses that are an exception to this rule.
Primary polydipsia is just too much water intake. These patients can usually make a very dilute urine (50-100 mOsm/kg) The kidney is an amazing organ that can excrete up to 20-30 liters a day. Hyponatremia with normal renal water excretion means the patient is drinking at least this amount each day. This might be seen in a trainee who is trying to “hydrate” before a road march.
The other two issues can occur with moderate intake but limited solute intake (<100 mOsm/day) and a dilute urine, this is beer potomania and tea and toast syndrome. Both beer and bread have low solute content, but any diet can cause this problem. These patients can make a dilute urine. The issue here is, with such low amount of solute in the diet, they cannot make much urine. Therefore the water is retained and sodium levels drop.
There is a situation where an elevated ADH is ‘appropriate’, even in the setting of hyponatremia. In this case it would be hypovolemic hyponatremia. This occurs when the intake of water exceeds the kidney’s ability to excrete it, resulting in a concentrated urine. If the blood volume is low, this will cause the release of ADH along with activation of the renin-angiotensin-aldosterone-system (RAAS). These patients are typically have the “dehydrated” look with lethargy, dry mucous membranes, oliguria, hypotension, tachycardia, overall can be shocky.
As mentioned urine will be extremely concentrated. It is not an impaired capacity to dilute the urine, but it’s ADH acting on the cells in the cortical collecting duct pulling water into the bloodstream.
Next, hyponatremia maybe seen in the hypervolemic patients. Two of these are chronically ill patients and one is a more acute presentation. Congestive heart failure (CHF) and decompensated cirrhosis can both create a hyponatremia. These patients are sick and difficult to manage.
In CHF, they patient may present with pulmonary, extremity edema, dyspnea, chest pain. The results of CHF are a decreased cardiac output, which in turn causes a decrease in the GFR. In an effort to compensate, the RAAS is activated, raising the blood pressure and increased sodium reabsorption. These effects also increase thirst and in the later stages of CHF, intake can exceed excretion.
Cirrhosis is another serious chronic condition. Patients may present with ascites, telangiectasias, icterus, jaundice, and oliguria. Other issues contributing include, vasodilation from hepatic congestion, portal hypertension, hypoalbuminemia. This leads to hypoperfusion of the kidney, decreased GFR, an increase in the RAAS activation, and increased sodium reabsorption. Many patients have poor oral intake and similar to CHF, they develop hyponatremia.
The more acute presentation is nephrotic syndrome. Nephrotic syndrome is caused by many things, but there is massive loss of protein, namely albumin. Albumin is not normally filtered through the glomerulus, but in nephrotic syndrome, it is lost to the urine. There is massive swelling and third spacing of fluid as the vessels lose their oncotic pressure. This results in decreased GFR and increased RAAS activation, with increased sodium reabsorption. Hyponatremia can develop. This is pretty rare and is unlikely to be seen.
Finally euvolemic hyponatremia all share some common features. Inappropriately increased ADH, impaired diluting capacity, and euvolemia.
Hyponatremia caused by adrenal insufficiency and Hypothyroidism is difficult and multifactorial. However, in euvolemic hyponatremia, at least test for these two diseases. Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH) may be a primary or secondary disorder with many possible etiologies. Often, this represents a very difficult disorder to treat. SIADH tends to be a diagnosis of exclusion: before diagnosing SIADH, adrenal insufficiency and hypothyroidism must be ruled out. These disorders are clinically indistinguishable from SIADH. Some of the causes of SIADH are listed:
- CNS Disorders: Infection: meningitis, encephalitis, abscess; Vascular: thrombosis, hemorrhage, vasculitis; Neoplasm: primary or metastatic; psychosis
- Drugs: intravenous cyclophosphamide, carbamazepine, vincristine or vinblastine, haloperidol, amitriptyline, SSRI’s: fluoxetine, sertraline
- Pulmonary Disease: lung cancer, pneumonia: viral, bacterial, fungal, Tuberculosis, Acute respiratory failure, Atelectasis, Asthma
Management of hyponatremia can be difficult as there are multiple approaches to this condition. In the setting of hypovolemic hyponatremia, the volume is replaced with isotonic solutions (0.9% sodium chloride or LR). Once the severe volume depletion has been corrected, ADH will be suppressed and the hyponatremia will correct.
Other variations of treatment for hypovolemic hyponatremia, which is not uncommon in the military is Marathon Runner’s Hyponatremia. This occurs because of solute losses in sweat may be quite large. The runner (or in this case the soldier) replaces these fluid losses with water or hypotonic fluid. Treatment includes administration of 100 mL 3% sodium chloride, this is usually when the sodium levels are below 120 mEq/L or have neurologic symptoms, including seizure.
Other options include:
- Fluid restriction
- Increased solute intake
- V2 receptor antagonists
- Conivaptan
- Tolvaptan
In hypervolemic hyponatremia management is usually a complex problem that is often resistant to medical management and may even require dialysis to treat.
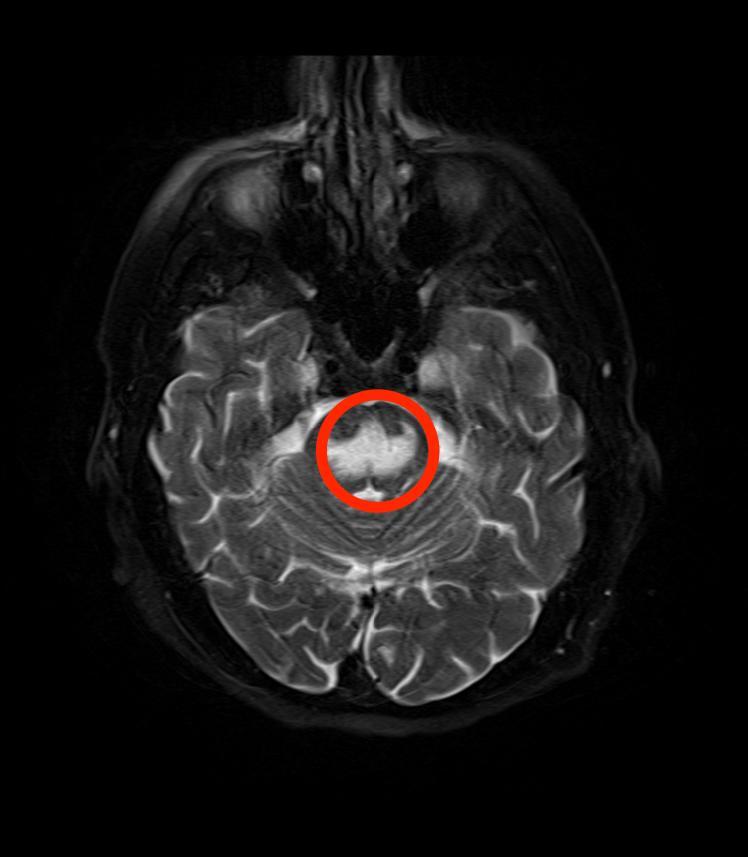
This is specifically relevant in the setting of euvolemic hyponatremia. The maximal rate of correction of the hyponatremia is extremely important and is particularly true in patients with chronic and/or longer duration hyponatremia. Rapid correction of hyponatremia can result in Osmotic Demyelination Syndrome (Central Pontine Myelinolysis), which is an irreversible and severe disorder impairing neurologic function.
The maximum rate of correction should be no more than 0.5 mEq/L per hour and no more than 12 mEq/L over the course of 24 hours. Additional treatments may be considered including:
- Administration of V2 receptor antagonist, for example tolvaptan or conivaptan.
- Removal of potential causes or modifiable factors impairing urine diluting capacity.
- Fluid restriction. In SIADH, this most commonly requires fluid restriction of less than 1000‐1500 mL per day.
Use of 0.9% normal saline should be a rare in the management of hyponatremia. Why you ask? Let’s review some background information. Hyponatremia is the most common electrolyte imbalance in the hospitalized patient. Intuitively, it may seem that giving 0.9% normal saline with an osmolality of 308 mOsm/kg would increase serum sodium because the serum osmolality is typically less than 280 mOsm/kg. Remember the normal is 275-295 mOsm/kg. This is an error in the understanding of hyponatremia and its management.
Here is the reasoning. Each liter of 0.9% sodium chloride has 154 mEq of sodium and 154 mEq chloride, equaling 308 mOsm of solute. The osmolality of 1 liter of NS is 308 mOsm/kg. The 308 mOsm of solute in each liter of NS will be excreted into the urine. For the purposes of this discussion, as long as the patient is in steady state (this is a chronic patient, so the body adjusted), then average solute intake in the form of intravenous fluid will equal the solute output in the urine.
Consider this, a patient with SIADH with a maximal urine diluting capacity of 411 mOsm/kg (this is as dilute as the patient can make urine). In this setting, the 308 mOsm of solute from the liter of 0.9% sodium chloride that this patient will excrete into the urine will be excreted at a urine osmolality of 411 mOsm/kg. This is because the patient’s maximal urine diluting capacity is at 411 mOsm/kg. This patient receives a 308 mOsm/kg intravenous fluid and excretes the 308 mOsm of solute in 750 mL of free water, which has an osmolality of 411 mOsm/kg.
The other 250 mL of free water that was in the original intravenous fluid is retained by the patient under the influence of ADH and/or all of the factors that are impairing urinary diluting capacity. This will continue to decrease serum Sodium concentration.
This is not an easy concept, so if it seems confusing, that is ok. Just know that in a patient with euvolemic hyponatremia, do not use 0.9% sodium chloride, as it may lower serum sodium concentration, rather than raise serum sodium concentration.

Leave a comment