
Originally posted on FOAMfrat: https://www.foamfrat.com/single-post/2018/09/05/Its-All-In-The-Hips
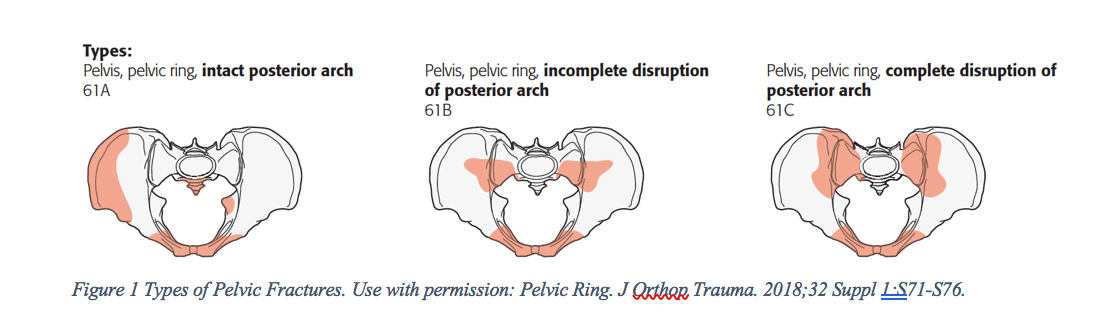
Pelvic fractures (PFs) can be one of the most devasting injuries. They can happen with simple falls in the elderly to the more prevalent young males involved in high energy motor vehicle accidents (MVA). PFs that arise from falls tend to be less severe as those in high energy trauma. They are classified using the Tile system—type A, B, or C with subtypes in each type, most important to know that type C is the most unstable (Figure 1) [1].
Stable pelvic fractures have mortality rates as high as 19%. Unstable PFs with hemodynamic instability only comprise about 1-4% of pelvic fractures and are characterized by disruption of the pelvis ring and associated with high energy blunt trauma [2]. However, they have a significantly high mortality rates, upwards of 40% [3,4]. Unstable PFs require rapid deceleration of at least 30 mph, there is often other pathology with this mechanism of injury [3].
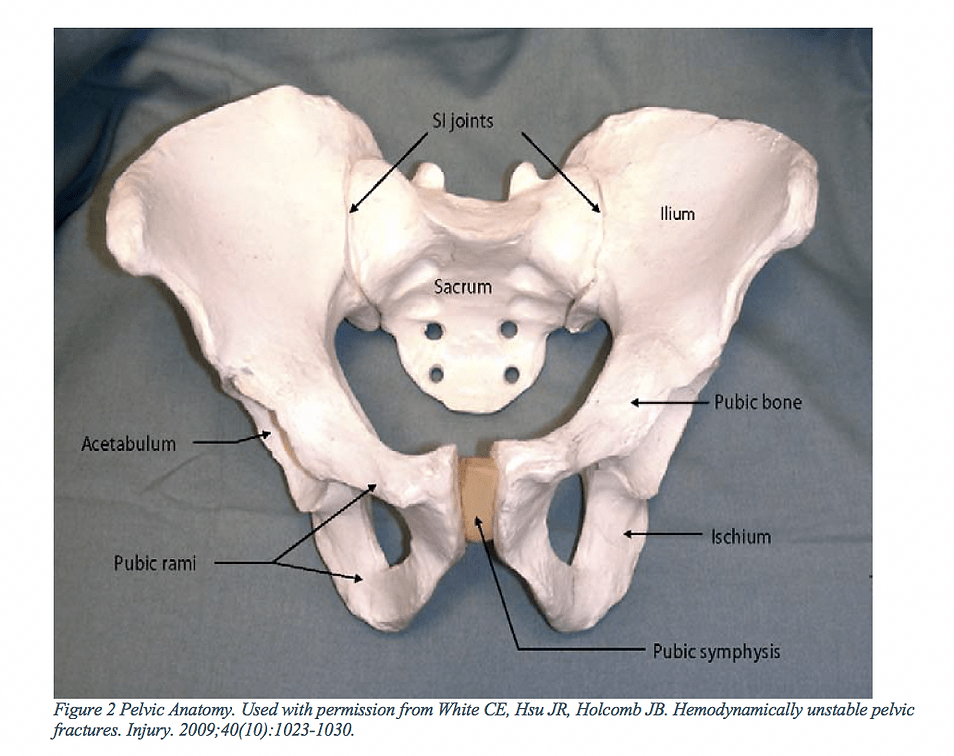
The pelvic girdle is comprised of three bones, the ischium, ilium, and pubis (Figure 2). The posterior of the pelvis is composed of the sacrum and ilium, to form—the sacroiliac joint. Anteriorly, the two pubic bones are joined at the pubic symphysis. These bony connections form a ring structure. While the symphysis is the weakest point of the pelvis, the SI joint is actually the strongest in the body.
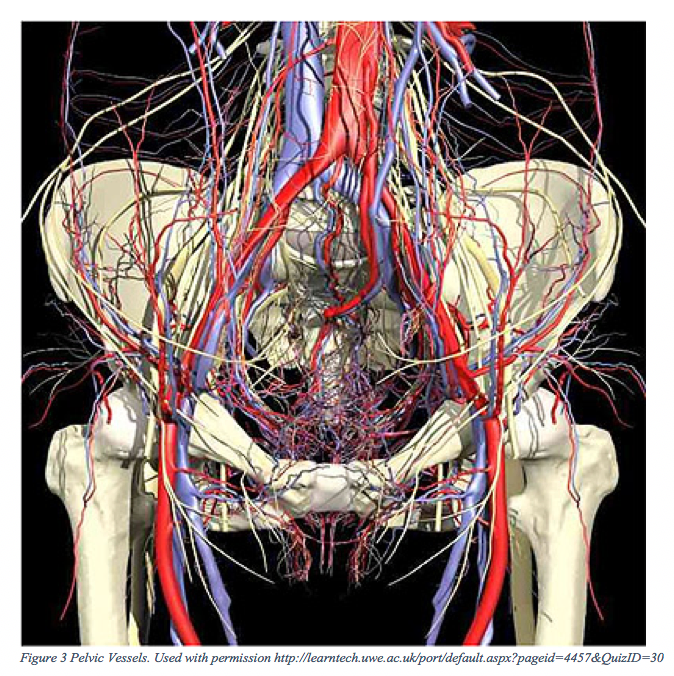
The bony pelvis is rich in blood supply (Figure 3), there are also several large caliber vessels that traffic through the area and provide blood supply to the several organs that lie within the cavity. Hemorrhage in unstable pelvic fractures come from the bone itself, arteries, and veins. Branches of internal iliac and sacral venous plexus are often the cause of death in unstable pelvic fractures [5].
With many ground ambulances lacking blood products, it is especially important to limit the blood loss. The use of crystalloids in trauma have deleterious effects6and should be limited if not all together withheld unless absolutely necessary. Both the stable and unstable pelvis can be splinted, however, it more important to splint the unstable PFs since they are associated with a high mortality rate. Pelvic binding is not a new concept, it’s been for many years in the emergency department and in EMS, the use of the bed sheet is an old but reliable method. Within the last 10 years there have been an increase in commercially available products.
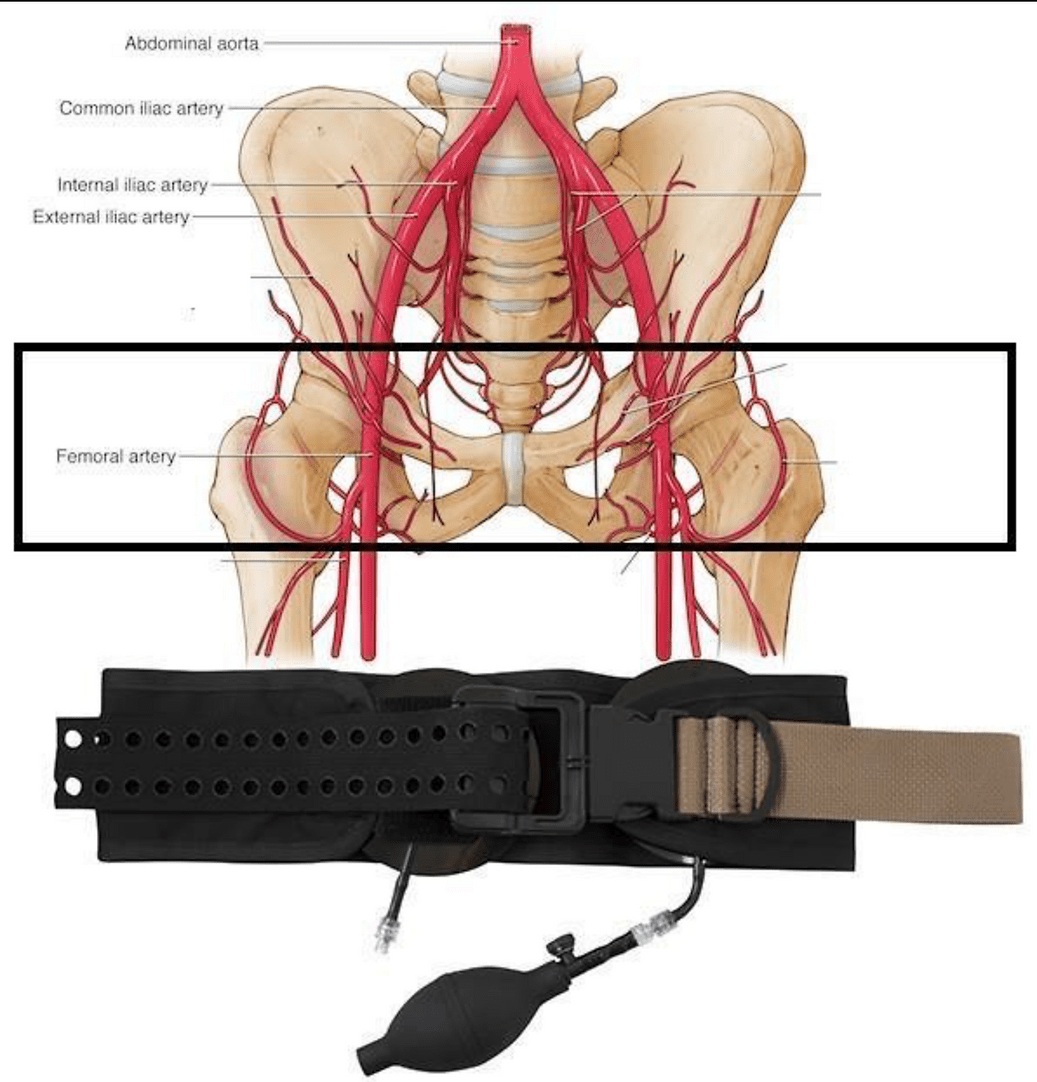
When splinting the pelvis, placement is critical. Many healthcare professionals incorrectly place a pelvic splint, rendering useless. Pelvic splints must be placed over the greater trochanters to be most effective. In obese patients, the bony landmarks may difficult to find.
Shackelford et al. reviewed the available data for the following devises for the Tactical Combat Casualty Care Guidelines (TCCC): Pelvic Binder™, T-POD®, and SAM Pelvic Sling®, and circumferential sheeting [7]. This review is probably the best data available on the prehospital use of pelvic binders.
They sought answers and found the following evidence:
-
Does a pelvic binder stabilize the pelvic fracture?
-
Only cadaver studies were available and recommended placement at the greater trochanters.Level of evidence: B
-
-
Does a pelvic binder control bleeding from a fractured pelvis?
-
With selection bias plaguing the data, there is weak evidence that they may reduce massive hemorrhage. Level of evidence: B
-
-
Does a pelvic binder improve survival?
-
Weak evidence is available to suggest it may improve survival.Level of evidence: C
-
-
Is there any harm in applying a pelvic binder?
-
There is little risk to the pelvic binder, possibly leaving it on too long. Level of evidence: C
-
-
What is the best type of pelvic binder?
-
There is no identified pelvic binder that demonstrated superior performance. Improvised pelvic binders have not been studied.Level of evidence: B
-
-
Where does pelvic binder fit into priorities?
-
Pelvic binders should be considered after addressing the immediate life threats or in the “circulation” period.
-
-
Who should get a pelvic binder?
-
Pelvic binders should be applied in suspected pelvic fractures with blunt or blast injuries and at least one of the following:
-
• Pelvic pain
• Any major lower limb amputation or near amputation
• Physical examination findings suggestive of a pelvic fracture
• Unconsciousness
• Shock
Interestingly, there was recognition of the Pneumatic Antishock Garment (PASG)in prehospital trauma where a pelvic fracture is suspected. There was a warning about the use of PASG and its potentially harmful effects.
None of the devices reviewed by Shackelford and colleagues can be used as both junctional hemorrhage control and pelvic splinting. There are two junctional tourniquets that can used as a pelvic splint: The Junctional Emergency Treatment Tool (JETT) and the Sam Junction Tourniquet (STQ) [8].
Individually, the in one case series, the T-POD demonstrated a raise the mean arterial pressure from 65.3 to 81.2 mmHg when applied in the ED. The SJT was used in a 16 patients clinical trial, resulting in an 9.9 % reduction of the pelvic distension [10].
One unique situation that one may encounter, is a pelvic fracture with an associated femur fracture(s). These injuries have a high mortality rate and are often associated with multi-system injury [7,14]. In these situations, splinting the pelvis with a binder should be the priority, and the use of a traction splint is most likely contraindicated [7]. It is best to make an effort to splint the thigh and femur to the other leg. Again, after applying the pelvic binder.
The evidence suggests pelvic binders do work for pelvic stabilization, however, it is still unknown if they can effectively control hemorrhage. If external hemorrhage is noted upon an exam, wound packing with the use of a JTQ would be indicated. It is recommended that they be employed in EMS in a similar fashion to the TCCC guidelines.
References:
1. Pelvic Ring. J Orthop Trauma. 2018;32 Suppl 1:S71-S76.
2. Wong JM, Bucknill A. Fractures of the pelvic ring. Injury. 2017;48(4):795-802.
3. Yoshihara H, Yoneoka D. Demographic epidemiology of unstable pelvic fracture in the United States from 2000 to 2009: trends and in-hospital mortality. J Trauma Acute Care Surg. 2014;76(2):380-385.
4. White CE, Hsu JR, Holcomb JB. Haemodynamically unstable pelvic fractures. Injury. 2009;40(10):1023-1030.
5. Martinelli T, Thony F, Declety P, et al. Intra-aortic balloon occlusion to salvage patients with life-threatening hemorrhagic shocks from pelvic fractures. J Trauma. 2010;68(4):942-948.
6. Yong E, Vasireddy A, Pavitt A, Davies GE, Lockey DJ. Pre-hospital pelvic girdle injury: Improving diagnostic accuracy in a physician-led trauma service. Injury. 2016;47(2):383-388.
7. Coccolini F, Stahel PF, Montori G, et al. Pelvic trauma: WSES classification and guidelines. World J Emerg Surg. 2017;12:5.
8. Carius BM, Fisher AD. Three Reasons Not to Use Normal Saline or Crystalloids in Trauma. JEMS. 2018.
9. Shackelford S, Hammesfahr R, Morissette D, et al. The Use of Pelvic Binders in Tactical Combat Casualty Care. J Spec Oper Med. 2017;17(1):135-147.
10. Lateef F, Kelvin T. Military anti-shock garment: historical relic or a device with unrealized potential? J Emerg Trauma Shock. 2008;1(2):63–69.
11. Kotwal RS, Butler FK, Jr. Junctional Hemorrhage Control for Tactical Combat Casualty Care. Wilderness Environ Med. 2017;28(2S):S33-S38.
12. Tan ECTH, van Stigt SFL, van Vugt AB. Effect of a new pelvic stabilizer (T-POD®) on reduction of pelvic volume and haemodynamic stability in unstable pelvic fractures. Injury. 2010;41(12):1239-1243.
13. Krieg JC, Mohr M, Ellis TJ, Simpson TS, Madey SM, Bottlang M. Emergent Stabilization of Pelvic Ring Injuries by Controlled Circumferential Compression: A Clinical Trial. J Trauma. 2005;59(3):659-664.
14. Willett K, Al-Khateeb H, Kotnis R, Bouamra O, Lecky F. Risk of mortality: the relationship with associated injuries and fracture treatment methods in patients with unilateral or bilateral femoral shaft fractures. J Trauma. 2010;69(2):405-410.

Leave a comment