
This article was last reviewed in February 2022 and is based on research available at that time. We will attempt to update this page as new evidence and best practice becomes available.
You may be aware of the recent resurgence in talk surrounding whole blood transfusions on the battlefield. There is quite a bit of stigma, myth, and misconception surrounding blood product administration by medics and corpsmen. This article is meant to enlighten military medics and corpsmen and arm them with facts when talking with their battalion PAs and Surgeons about Fresh Whole Blood (FWB). Hopefully, we can challenge the dogmatic approach to resuscitation in favor of some good evidence-based medicine.
Step 1: Read the Literature
Decisions in medicine are made, in large part, based on the evidence presented in scientific medical literature. The thing that will best help you discuss whole blood with your medical director is to know it yourself. Take the time to find and read the articles linked below each answer. You may also want to avail yourself of the basic sciences here and the continuing education resources here.
Frequently Asked Questions
Q: Why are we having this conversation?
A: In 2014 the JTS Committee on Tactical Combat Casualty Care, recommended whole blood as the resuscitation fluid of choice. Fresh Whole Blood (FWB) is blood collected from donors and immediately transfused into a patient without processing or storage. FWB is the fluid of choice for battlefield resuscitation of traumatically hypovolemic patients. FWB has been used by the U.S. Military since World War I and more recently in Combat Support Hospitals (CSH), Forward Surgical Teams (FST), Forward Resuscitative Surgery Systems (FRSS), and even aircraft carriers at sea. Also called Walking Blood Banks (WBB), these organizations have been drawing and transfusing whole blood into wounded patients since the beginning of the war. Recent medical research has provided evidence of the safety, efficacy, and benefits of collecting and transfusing whole blood in the field for Remote Damage Control Resuscitation (RDCR). Any delay in massive transfusion is associated with prolonged time to achieve hemostasis and an increase in mortality. Regardless of whether you are using component blood products or whole blood, the odds of mortality increase approximately 5% with each minute blood is delayed. Training for the use of FWB improves overall survival and reduces disability.
- Fresh Whole Blood Transfusion: Military and Civilian Implications (Crit Care Nurse, 2016)
- Warm Fresh Whole Blood Is Independently Associated With Improved Survival for Patients With Combat-Related Traumatic Injuries (J Trauma, 2009)
- Comparison of platelet transfusion as fresh whole blood versus apheresis platelets for massively transfused combat trauma patients. (Transfusion, 2011)
- Every minute counts: Time to delivery of initial massive transfusion cooler and its impact on mortality. (J Trauma Acute Care Surg, 2017)
Q: What are the indications for FWB transfusion?
A: FWB is the preferred fluid for resuscitation of suspected hemorrhagic shock in the traumatically injured patient. FWB is ideal for anemic, acidotic, hypothermic, coagulopathic patients with life-threatening traumatic injuries in hemorrhagic shock.
From the TCCC guidelines:
- Assess for hemorrhagic shock (altered mental status in the absence of brain injury and/or weak or absent radial pulse).
- IV/IO Access
- Intravenous (IV) or intraosseous (IO) access is indicated if the casualty is in hemorrhagic shock or at significant risk of shock (and may therefore need fluid resuscitation), or if the casualty needs medications, but cannot take them by mouth.
- An 18-gauge IV or saline lock is preferred.
- If vascular access is needed but not quickly obtainable via the IV route, use the IO route.
- Tranexamic Acid (TXA)
- If a casualty will likely need a blood transfusion (for example: presents with hemorrhagic shock, one or more major amputations, penetrating torso trauma, or evidence of severe bleeding)
OR
- If the casualty has signs or symptoms of significant TBI or has altered metal status associated with blast injury or blunt trauma”
- Administer 2 gm of tranexamic acid via slow IV or IO push as soon as possible but NOT later than 3 hours after injury.
Fluid resuscitation
- Assess for hemorrhagic shock (altered mental status in the absence of brain injury and/or weak or absent radial pulse).
- The resuscitation fluids of choice for casualties in hemorrhagic shock, listed from most to least preferred, are:
1. Cold stored low titer O whole blood
2. Pre-screened low titer O fresh whole blood
3. Plasma, red blood cells (RBCs) and platelets in a 1:1:1 ratio
4. Plasma and RBCs in a 1:1 ratio
5. Plasma or RBCs alone
NOTE: Hypothermia prevention measures [Section 7] should be initiated while fluid resuscitation is being accomplished.
If not in shock:
- No IV fluids are immediately necessary.
- Fluids by mouth are permissible if the casualty is conscious and can swallow.
If in shock and blood products are available under an approved command or theater blood product administration protocol:
- Resuscitate with cold stored low titer O whole blood, or, if not available
- Pre-screened low titer O fresh whole blood, or, if not available
- Plasma, RBCs, and platelets in a 1:1:1 ratio, or, if not available
- Plasma and RBCs in a 1:1 ratio, or, if not available
- Reconstituted dried plasma, liquid plasma or thawed plasma alone or RBCs alone
- Reassess the casualty after each unit. Continue resuscitation until a palpable radial pulse, improved mental status or systolic BP of 100 mmHg is present.
- Discontinue fluid administration when one or more of the above end points has been achieved.
- If blood products are transfused, administer one gram of calcium (30 ml of 10% calcium gluconate or 10 ml of 10% calcium chloride) IV/IO after the first transfused product.
Given increased risk for a potentially lethal hemolytic reaction, transfusion of unscreened group O fresh whole blood or type specific fresh whole blood should only be performed under appropriate medical direction by trained personnel.
Transfusion should occur as soon as possible after life-threatening hemorrhage in order to keep the patient alive. If Rh negative blood products are not immediately available, Rh positive blood products should be used in hemorrhagic shock.
If a casualty with an altered mental status due to suspected TBI has a weak or absent radial pulse, resuscitate as necessary to restore and maintain a normal radial pulse. If BP monitoring is available, maintain a target systolic BP between 100-110 mmHg.
Reassess the casualty frequently to check for recurrence of shock. If shock recurs, re-check all external hemorrhage control measures to ensure that they are still effective and repeat the fluid resuscitation as outlined above.
Refractory Shock
- If a casualty in shock is not responding to fluid resuscitation, consider untreated tension pneumothorax as a possible cause of refractory shock. Thoracic trauma, persistent respiratory distress, absent breath sounds, and hemoglobin oxygen saturation < 90% support this diagnosis. Treat as indicated with repeated NDC or finger thoracostomy/chest tube insertion at the 5th ICS in the AAL, according to the skills, experience, and authorizations of the treating medical provider. Note that if finger thoracostomy is used, it may not remain patent and finger decompression through the incision may have to be repeated. Consider decompressing the opposite side of the chest if indicated based on the mechanism of injury and physical findings
You should consider the condition of your patient and your tactical situation. If you expect any delay in evacuation or your patient has extensive injuries and has already lost a significant amount of blood, the sooner you initiate the transfusion, the more likely they will survive.
- TCCC Guidelines for Medical Personnel (November 2020)
- Fresh whole blood transfusions in coalition military, foreign national, and enemy combatant patients during Operation Iraqi Freedom at a U.S. combat support hospital (World J Surg, 2008)
Q: Can regular medics perform blood administration?

A: Yes. Administration of Blood Products is already a 68W MOS task in STP 8-68W13-SM-TG (CAC Required). Task 081-835-3000 Administer Blood (Skill Level 3) was written for blood component administration, but is readily adaptable to FWB. Minimal additional training is needed to safely perform FWB collection and transfusion in the field. FWB transfusion is currently taught to new medics during AIT. Conventional units across the military are currently implementing their own versions of the 75th Ranger Regiment’s ROLO program. Some civilian EMS agencies have even started using Cold Stored Type-O Low Titre Whole Blood for fluid resuscitation of patients in hypovolemic shock.
Q: What makes FWB so great?

A: Whole blood has all of the red blood cells, clotting factors, and platelets that the patient needs to be resuscitated all in one bag, all transfusing at the same time. When a patient has lost enough blood to be in shock, what they need most is blood back in their body. There is some controversy surrounding the degradation of stored blood components. These concerns do not apply to fresh whole blood.
- Fresh versus old blood: are there differences and do they matter? (Hematology, 2013)
- Whole blood: the future of traumatic hemorrhagic shock resuscitation (Shock, 2014)
- Blood far forward: Time to get moving! (JTACS, 2015)
- Whole blood for hemostatic resuscitation of major bleeding. (Transfusion, 2016)
Q: What is wrong with how we have been doing things?
A: For decades the standard was to infuse large quantities of saline into the hypovolemic trauma patient. Saline is acidic with a pH around 5.5. Saline boluses do not increase blood pressure in a useful way. Saline is often stored at ambient temperatures and is commonly not warmed before administration (which as it turns out being cold is the only way saline significantly effects blood pressure).
Within the first few years of the current conflicts, we realized that we were causing preventable death and disability associated with diluting the oxygen-carrying and clotting capabilities of the body (called dilutional anemia). Furthermore, over-resuscitating a patient with crystalloids has been shown to contribute to pulmonary dysfunction at the 3-day mark.
The common standard for massive transfusions in large hospitals is a 1:1:1 ratio of packed red blood cells (pRBC), fresh frozen plasma (FFP), and platelets. Smaller facilities like Forward Surgical Teams (FST) and medical evacuation platforms like Pedro (U.S. Air Force PJs) and DUSTOFF (Conventional Army MEDEVAC), and MERT (U.K. Army Medical Emergency Response Team) tend to only have pRBC and FFP, but not platelets, due to the logistical burden. Currently, platelets have a five-day shelf life, must be stored at room temperature and oscillated. Studies show that FWB has similar benefits to the standard 1:1:1 transfusion protocol. In austere environments where standard blood products are unavailable, FWB is a viable alternative.
- Cold and warm infusion of Ringer’s acetate in healthy volunteers: the effects on haemodynamic parameters, transcapillary fluid balance, diuresis and atrial peptides. (Acta Anaesthesiol Scand, 1993)
- Haemodynamic effects of cold versus warm fluid bolus in healthy volunteers: a randomised crossover trial. (Crit Care Resusc, 2018)
- Fresh whole blood use by forward surgical teams in Afghanistan is associated with improved survival compared to component therapy without platelets. (Transfusion, 2013)
- Lethal injuries and time to death in a level I trauma center. (J Am Coll Surg, 1998)
- Initial severity of metabolic acidosis predicts the development of acute lung injury in severely traumatized patients. (Crit Care Med, 2000)
- Comparison of platelet transfusion as fresh whole blood versus apheresis platelets for massively transfused combat trauma patients (Transfusion, 2011)
Q: Why not just use Freeze Dried Plasma (FDP)?

A: Freeze-dried plasma is much better than saline for fluid resuscitation because it isn’t acidic and it doesn’t dilute clotting factors. Although it is not FDA-approved yet, it has been given a provisional approval for military use and has been used by U.S. Special Operations Forces overseas with great results. Our French counterparts have been using it since the 90’s.
However, FDP doesn’t replace the oxygen-carrying red blood cells in FWB. There have been no controlled trials studying this, but data from WWII indicates increased survival once the U.S. switched from bottles of plasma to group O whole blood. The switch was credited by the Surgeons General of the Army and Navy as being the greatest lifesaver of World War II.
“Plasma gives more time to get whole blood into the patient. ”
– HK Beecher, WWII
FDP should be used as a fluid resuscitation adjunct while FWB is being collected for transfusion.
Q: Isn’t blood transfusion a risky procedure?
A: If done properly, FWB transfusion has a very good risk to benefit ratio. All medical procedures have an inherent level of risk if done carelessly or incorrectly. The main thing that most folks are concerned with is transfusion reactions. There is a 1:80,000 chance of transfusion reaction with matched blood types, and a 1:120,000 chance of a reaction with matched plasma. The reactions, if seen, are commonly mild and range from pain at the injection site, to rash and fever. In any case, there does not appear to be any increased risk of morbidity or mortality from infusing incompatible plasma. These are not commonly noticeable outside of a well-controlled transfusion center. Even in major trauma centers, most physicians aren’t concerned with flushing and pruritus while resuscitating the trauma patient.
Less likely but more severe reactions include acute hemolytic anemia (AHA), transfusion-related acute lung injury (TRALI), and transfusion-related circulatory overload (TACO). Medics should know how to identify and treat these reactions, but should not delay resuscitation because it might cause a reaction.
The worst kind of transfusion reaction is known as Transfusion Related Graft vs. Host Disease (tGVHD). It is exceedingly rare, there is no way to test for it, and if your patient gets it there is no treatment. There has been only one documented case of tGVHD in more than 10,000 military FWB transfusions.
- Risks associated with fresh whole blood and red blood cell transfusions in a combat support hospital (Crit Care Med, 2007)
- Incompatible type A plasma transfusion in patients requiring massive transfusion protocol: Outcomes of an Eastern Association for the Surgery of Trauma multicenter study (J Trauma Acute Care Surg, 2017)
Q: What about Rh factor reactions?
A: A mismatch in the Rhesus (Rh) D antigen doesn’t cause an immediate hemolytic reaction after the first exposure and is nearly irrelevant in the emergency prehospital setting. According to the American Red Cross, 10-20% of the U.S. population does not have the Rh D antigen on the surface of their red blood cells, also known as Rh “negative”. After exposure to Rh “positive” blood, around 20-26% will develop a sensitivity within four weeks. However, only 3-4% will develop a strong immune response to a future administration. While it is common practice to give women of childbearing age Rh-negative blood, if it isn’t available, Rh-positive whole blood should be transfused as it’s still preferred over colloid or crystalloid infusion.
- Safety of uncrossmatched type-O red cells for resuscitation from hemorrhagic shock. (J Trauma, 2005)
- Rhesus Negative Woman Transfused With Rhesus Positive Blood: Subsequent Normal Pregnancy Without Anti D production (Ghana Med J, 2015)
- Emergency transfusion of patients with unknown blood type with blood group O Rhesus D positive red blood cell concentrates: a prospective, single-centre, observational study. (Lancet, 2017)
Q: What about blood-borne diseases?
A: FWB is meant to be taken from a U.S. service member and given to a battlefield casualty. This allows the donor to be screened for common transmissible diseases. Additionally, the risk of infectious disease transmission with FWB transfusion can be minimized by rapid screening tests for HIV, hepatitis B (HBV), hepatitis C (HCV), malaria, and syphilis (RPR) before transfusion. During the wars in Iraq and Afghanistan, there have been over 10,000 fresh whole blood transfusions. Of those, there has been one case of hepatitis C and one case of tGVHD which resulted in the death of the recipient.
Q: Isn’t “A to A, and O for everyone else” reckless?
A: There is an extremely low risk of lethal transfusion reaction from FWB. The unqualified success of the Ranger O Low-titer (ROLO) Whole Blood Program uses low titer group O whole blood for every casualty on the battlefield.
However, in cases of small teams or low numbers of group O donors, the mnemonic “A to A and O to everyone else” may a safe option. During WWII, almost all transfusions were group O whole blood, regardless of titer or the patient’s blood group. The very nature of the conditions in which FWB transfusion takes place doesn’t lend itself to a well-controlled trial. About 80% of the population is either type-A or type-O. The remaining 20% is divided between types-B and -AB. While the chances of a reaction are higher in this 20%, the rate is still low and the effects tend to be mild. If faced with the choice between possible mild transfusion reaction and likely or certain death from hemorrhagic shock, the choice is clear. Trying to find an exact whole blood match for group B and AB patients may cause an unacceptable delay in care.
- Tactical Damage Control Resuscitation (Mil Med, 2015)
-
Low titer group O whole blood resuscitation: Military experience from the point of injury (JTACS, 2020)
Q: Does taking blood from a healthy Soldier put them at risk during combat?
A: No. There is no significant decrease in either physical or in shooting performance after donating 1 unit (450mL) of whole blood. Studies show buddy transfusion is feasible for healthy well-trained soldiers and does not decrease donor combat performance under ideal circumstances.
- Donor performance of combat readiness skills of special forces soldiers are maintained immediately after whole blood donation. (Transfusion, 2013)
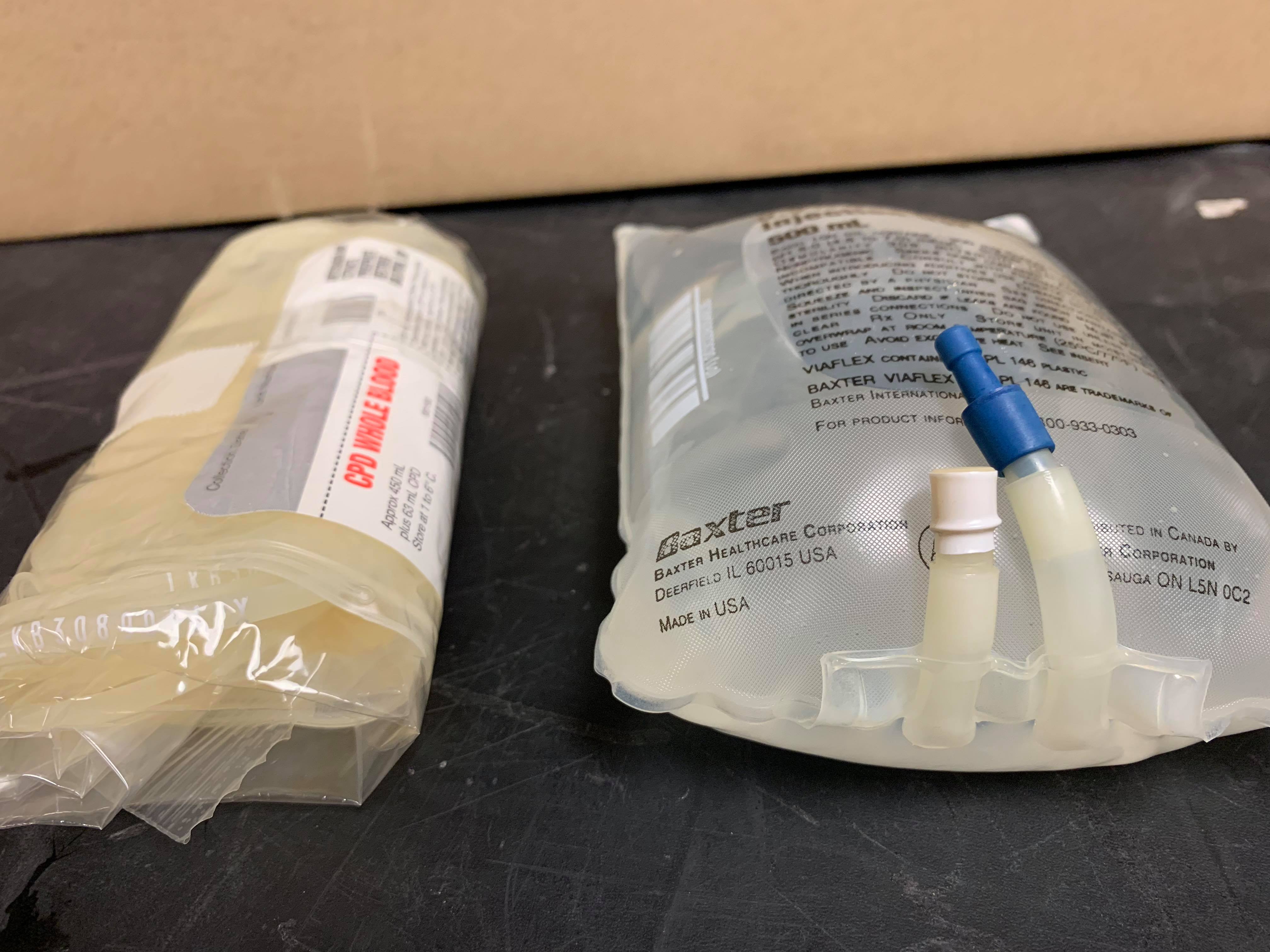
Q: How much equipment is needed?
A: Less than the volume and weight of a 500mL saline bag.

Q: Can trained non-medical personnel perform whole blood collection?
A: Yes. Non-medical personnel can start whole blood collection provided they are well trained and are able to practice frequently. The 75th Ranger Regiment trains Advanced Ranger First Responders to collect FWB from pre-designated donors. Your success will depend on how well trained and practiced your CLS are.
Q: Can I just use Dog Tags to select donors?
A: You probably shouldn’t. Military ID tags do have the blood type on them but are subject to an error rate. They can be used to identify potential donors but confirmatory testing with a rapid blood typing system, such as an Eldon Card should be used. A much better option is to screen and identify donors before deployment. Using rapid blood typing cards or military issued ID tags to determine blood types should be your last resort.
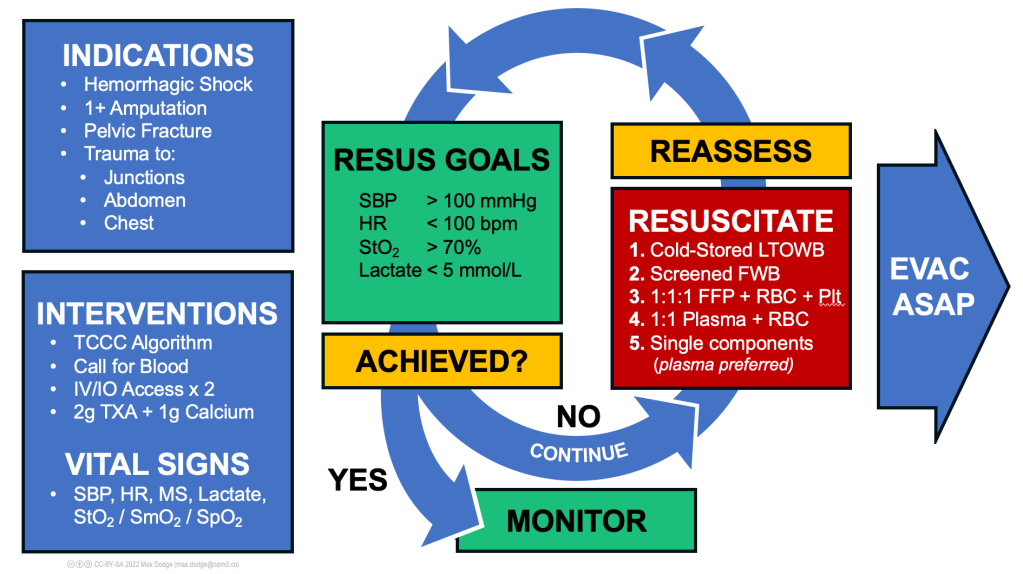
Q: Is it possible to overdose on FWB?
A: You should administer fluid resuscitation to meet a set of goals. Under the most austere of conditions, give blood or FDP until you see a positive change in mental status or can feel a radial pulse. If you have the time and equipment, you should resuscitate to meet other vital signs goals, whether that is MAP, heart rate and systolic pressure, tissue oxygenation, or lactate. Over-resuscitation with any fluid can cause poor outcomes.
Created by Max Dodge (max.dodge@opmd.co) and Andrew D. Fisher
Creative Commons License CC-BY-SA (https://creativecommons.org/licenses/by-sa/2.0/)
Specifically for the administration of blood products is the issue of hypocalcemia. Blood is collected in bags containing sodium citrate. Sodium citrate prevents the blood’s clotting cascade from activating in the bag prior to administration. Each unit of blood contains approximately 3 grams citrate, which binds with calcium in the body to deactivate the natural clotting mechanisms. The healthy adult liver will metabolize 3 grams of citrate about every 5 minutes. However, transfusion above this rate, with an impaired liver, or into an already acidotic patient can lead to citrate toxicity and hypocalcemia. This hasn’t been shown to have an effect on clotting, but it can cause some mild to moderate side effects such as muscle tremors or spasms (tetany), hypotension, or allergic reaction (urticaria). This can all be treated or avoided with the administration of calcium gluconate after the first unit of FWB.
- Citrate metabolism in blood transfusions and its relationship due to metabolic alkalosis and respiratory acidosis (Int J Clin Exp Med, 2015)
- Citrate Toxicity During Massive Blood Transfusion (Transfusion Med Rev, 1988)
Q: What if I don’t use the blood I collected?
A: FWB can be stored at room temperature for up to 8 hours and then refrigerated after that for up to 21 days. Generally speaking though, if you don’t use it in 24 hours, it’s probably not an emergency and you can dispose of it. If you hand your patient off to another level of medical provider, unless they have access to type-specific blood products, you should give them the blood you’ve collected. MEDEVAC personnel have already been transfusing blood products in the field for years and should be very familiar with how to proceed. During one MASCAL aboard a Navy ship, excess blood was transfused back into the donors.
- Red tides: Mass casualty and whole blood at sea (J Trauma Acute Care Surg, 2018)
Q: How do I train for field FWB transfusion?
A: Gather supplies. You can find FWB Transfusion kits from both Chinook and Boundtree. You can also buy the components in bulk to save money. The THOR Network has published a free online Whole Blood Field Transfusion Course. Read through the article published by members of the NGCM in the Journal of Trauma and Acute Care Surgery (accessible with your AMEDD Virtual Library OpenAthens account). Reserve classroom space and ensure you have the support of your Surgeon and PA.
- Conducting fresh whole blood transfusion training. (J Trauma Acute Care Surg, 2019)
- Prolonged Field Care – Podcast Episode 36: ROLO to SOLO: The Logistics of Fresh Whole Blood Transfusion (2018)
- Joint Trauma System (JTS) Fresh Whole Blood Clinical Practice Guideline (2005)
Q: Is there a presentation that I can use to teach damage control resuscitation and whole blood transfusions?
A: Yes, here it is. Fresh Whole Blood Training Presentation.
Additional Resources for Gettin’ Smart
Fresh Whole Blood Transfusion “FAQ’s” in Prolonged Field Care (LTC Andrew Cap, 2014)
Medscape – Rh Incompatibility (Salem, Lo, 2017)

Ranger Whole Blood Program wins an Army’s Greatest Innovation Award (Maj. Tony Mayne, 2017)
Trauma Hemostasis & Oxygenation Research (THOR)
(PODCAST) PJ Medcast #54: The Ranger Blood Program (2016)
(FOAM) Life in the Fastlane – Citrate Toxicity
(PODCAST) Blood Bank Guy Episode 40: “Wholly Whole Blood!” with Mark Yazer (2017)
(PODCAST) Austin-Travis County EMS System Office of the Medical Director – Episode 12: Trauma Resuscitation (2018)

Leave a comment